Arm Pump and Motocross
Jondy L. Cohen, M.D.
Stanislaus Orthopaedic & Sports Medicine
Clinic
Arm Pump:
Medicines Neglected Syndrome
A debilitating condition is limiting the performance of
some of the world's top athletes. This condition affects
competitors regardless of age, sex, or race, and varies in
severity from slightly annoying to downright dangerous.
"Chronic Exertional Compartment Syndrome of the Forearm", the
most common cause of "arm pump", lacks large foundations and
other sources of funding and therefore little research is
conducted on the subject. Although the world's governments are
not racing to cure arm pump, the editors of Motocross Action want to help you sort fact from fiction, opinion from
knowledge, and quackery from cure. Motocross Action contacted
me, a practicing Orthopaedic Surgeon in Northern California,
to define the current status of arm pump.
Although you have probably heard of arm pump it is unlikely
that your doctor has. I extensively reviewed the medical
literature and found almost nothing on this subject. In the
"American Journal of Sports Medicine" in 1998 one author even
states that "Chronic compartment syndromes of the upper
extremity are rare, and only a few cases have been reported in
the literature." A casual sampling of my sports medicine
colleagues revealed only one that was familiar with the
disorder. Conversely, almost every rider over adolescence that
I contacted was not only familiar with the condition, but also
aware of the existence of a surgical treatment and usually
several nonoperative treatments. The fact that several
national level pros have recently undergone surgery for arm
pump has heightened interest in this condition.
 Riders suffering from arm pump often look for an
easy fix. These folks don't want to put much effort into
understanding the problem and would prefer that I propose a
quick operation, medication, or corrective therapy. This
attitude is common in many of my patients, regardless of the
diagnosis. We Americans have become used to easy, drive
through, technologically advanced solutions to life's
problems. It's not surprising that we expect a modern, once a
day, HMO covered, FDA approved, arthroscopic, computer
controlled and laser guided, medical solution to arm pump.
Unfortunately, the best way for you to treat your arm pump is
to understand the cause of arm pump. Just like questions
concerning jetting and suspension, no simple one-sentence
answer is adequate. If you're a successful competitor lacking
a factory mechanic then you have likely read volumes about
jetting and suspension. If arm pump sometimes slows you down
read on. Riders suffering from arm pump often look for an
easy fix. These folks don't want to put much effort into
understanding the problem and would prefer that I propose a
quick operation, medication, or corrective therapy. This
attitude is common in many of my patients, regardless of the
diagnosis. We Americans have become used to easy, drive
through, technologically advanced solutions to life's
problems. It's not surprising that we expect a modern, once a
day, HMO covered, FDA approved, arthroscopic, computer
controlled and laser guided, medical solution to arm pump.
Unfortunately, the best way for you to treat your arm pump is
to understand the cause of arm pump. Just like questions
concerning jetting and suspension, no simple one-sentence
answer is adequate. If you're a successful competitor lacking
a factory mechanic then you have likely read volumes about
jetting and suspension. If arm pump sometimes slows you down
read on.
Forearm pain that occurs while riding is not always due to
arm pump. Riders with carpel tunnel syndrome, ganglion cysts,
arthritis, neck abnormalities, tennis elbow, and fractures
have all complained of forearm pain while riding. In the
interest of brevity I will only discuss arm pain due to
Chronic Exertional Compartment Syndrome of the Forearm
(CECSF). Please remember, this article cannot substitute for a
good physical exam by a physician. Since I am writing about a
condition and I haven't examined you, then maybe this isn't
your condition. Your physician should be able to help.
The Heartbreak of Arm Pump
Severe arm pump can ruin a great day. A talented racer may
meticulously prepare his bike and his body, spending thousands
of dollars and countless hours, for the last race of the
Winter Solstice Shootout Amateur National. He knows that this
is the most important race of his life and that none of his
competition is as prepared as he. This is HIS year to shine.
Ignoring his pre-gate jitters he takes the holeshot and leads
for several laps before his forearm muscles painfully enlarge
and harden. His hands become useless and finger movement just
adds to the hurt. He may hang on pitifully while his pace
drastically slows. Eventually, with competitors passing at
will, he exits the track, the day having lost its allure.
Not all cases of arm pump are as severe as this example.
Often patients complain that they can ride trails all day
without arm pump on one week and then pump up quickly at the
track the next week. Symptoms usually occur at the palm side
(volar) of the forearm rather than the back side (dorsal
side). Numbness or tingling in the forearm and hand can occur.
Fortunately, the symptoms of arm pump are temporary and hand
function quickly returns after a short rest.
Acute Compartment Syndrome is Not Arm
Pump
Persistent or progressive symptoms despite resting are
worrisome and may indicate the start of a rare condition
called "Acute Compartment Syndrome". Unlike the chronic form
(arm pump), symptoms of acute compartment syndrome increase
even after resting. The acute form usually results from an
injury, but may occur after strenuous exercise. Acute
compartment syndrome is a true emergency and may lead to
permanent muscle damage unless surgically treated in less than
6-8 hours. If you cannot move your fingers 15 minutes after
you stop riding be concerned and perform the following test.
Have a friend move your fingers for you in both directions
(flexion and extension). If this maneuver results in severe
pain, go to a doctor. If your pain continues or increases
long after riding stops seek medical attention at once! If
you have acute compartment syndrome don't assume it's just arm
pump, unless you like the moniker Lefty (or Righty).
Muscles and Two Stroke Engines
Understanding arm pump begins with understanding muscles.
Muscles, like two stroke engines, burn fuel and oxygen to
produce horsepower, exhaust, and heat. But, the motor between
your legs (I mean your bike, stud) differs in some important
ways from the motor inside your legs (your leg muscles).
Engines use air to transport intake and exhaust; the
air/fuel mixture is made in the carburetor and carried as gas
through the intake and transfer ports to the cylinder. The
signal to burn this mixture initiates in the ignition and is
carried by the spark plug wire to the plug. The burning gas
expands forcefully pushing the piston down. This energy then
progresses through the transmission and chain, to the rear
wheel. Exhaust is sent through the exhaust port and out the
pipe.
Muscles use blood to transport intake and exhaust; the
blood/oxygen/fuel mixture is made in the lungs, and carried by
blood through arteries (intake ports) and capillaries
(transfer ports) to every tiny fiber in the muscle. (Figure
1). The signal to burn this mixture initiates in the brain
(the ignition) and is carried by nerves (the plug wire). The
burning occurs at every muscle fiber (the cylinders), causing
them to either shorten or resist lengthening, depending on the
amount of force pulling against it. Energy then progresses
from muscle to tendon to bone. Exhaust leaves each muscle
fiber by entering the bloodstream in capillaries that empty
into veins. 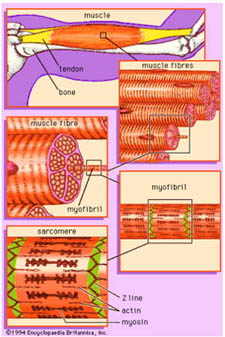 Veins bring exhaust filled blood back to
the heart that pumps it to the lungs. In the lungs blood
releases carbon dioxide and binds oxygen. (A more complete but
longer explanation of this process is provided in the sidebar
titled "More About Muscles".) Veins bring exhaust filled blood back to
the heart that pumps it to the lungs. In the lungs blood
releases carbon dioxide and binds oxygen. (A more complete but
longer explanation of this process is provided in the sidebar
titled "More About Muscles".)
Muscles are often
found together in "fascial compartments". Fascial compartments
contain muscle wrapped in a layer of "fascia". Fascia, a tough
but thin white gristle, envelops the compartment like a casing
wraps a sausage. Fascia helps to both anchor muscles and to
give them form. Fascia is very strong but it is not very
elastic. The inelasticity of fascia surrounding muscle
means that even small increases in the volume of a fascial
compartment can cause big pressure increases within the
compartment.
Forearm Design
The forearm has two sides, the palm side (called the
"volar" side), and the backside (called the "dorsal side").
The muscles on the palm side of the forearm bend (flex) the
fingers and wrist. The muscles on the backside of the forearm
straighten (extend) the fingers and wrist. When you grab your
bars notice how the muscles on both sides of the forearm
tighten. The palm muscles are bending your fingers to grip the
bars and the backside muscles are holding your wrist stable.
Figure 2 shows the volar (palm) side and the dorsal (back)
side of a forearm. Notice the muscle fibers (red) turning into
tendons (white) before crossing either the elbow or wrist.
Also notice that the fascia is removed in these photos in
order to better see the muscles.

Figure 2: The palm side (left) and the back
side (right) of a forearm. Notice the muscle fibers (red)
turning into tendons (white) before crossing either the elbow or wrist. (Fascia
has been removed.)
Figure 3 shows a crosscut section of forearm. The forearm
has four fascial compartments that I have colored: 1.In pink
are the muscles of the superficial volar compartment, 2. In
orange are the muscles of the deep volar compartment, 3. In
red are the muscles of the dorsal compartment, and 4. In
yellow are the muscles of the mobile wad compartment. Usually
only the two compartments on the palm side of the forearm,
purple and orange (the superficial and deep volar
compartments) pump up.
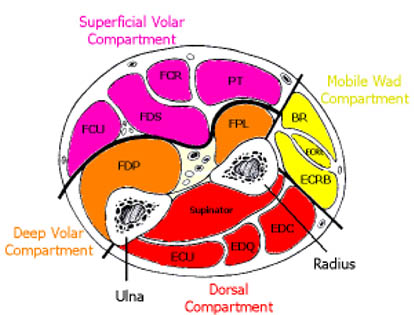
Figure 2 Cross section of a forearm. Palm
up.
How Arm Pump Happens
During vigorous exercise muscles require a tremendous
amount of oxygen rich blood and commonly increase in volume by
up to 20%. The engorged muscle inside the inelastic fascia
results in increasing pressure within the compartment.
Although gases and solids are compressible, fluids are not.
The incompressible fluid within the inelastic facia makes the
forearm feel hard as bone. (A similar mechanism is used
elsewhere in the body to create a rigid structure out of soft
tissue.) If the "compartment pressure" rises high enough,
blood vessels can collapse which restricts or stops the flow
through that vessel. Veins, with their low pressure and thin
walls, collapse earlier than high pressure, thick walled,
arteries. When venous flow reduces, arterial blood continues
to enter the fascial compartment but is restricted from
leaving. This restricted outflow further increases the
compartment pressures. If the compartment pressure rise higher
than the pressure in the capillaries (the "capillary
pressure") or even the arteries (the "arterial pressure") then
these vessels may collapse and result in "muscle ischemia" - a
painful condition of oxygen deprivation. Muscle ischemia leads
to even higher compartment pressures via pathways we won't
discuss here. This cycle of increasing pressure is depicted in
Figure 3.
The scenario described above is a well-documented condition
that occurs occasionally in the lower legs of distance
runners. A few cases have been described in the hands, feet,
thigh, elbow, and forearm. The condition is called various
names including chronic compartment syndrome, effort-related
compartment syndrome, exercise-induced compartment syndrome,
and chronic exertional compartment syndrome. When it occurs in
the forearm I refer to this condition as "chronic compartment
syndrome of the forearm". (CCSF) All of these names seek to
differentiate this condition from the much more dangerous
syndrome of "acute compartment syndrome". (See Acute
Compartment Syndrome above.)
Despite what the medical literature says, we all know that
chronic compartment syndrome of the forearm in motocrossers is
common. It is probably more common than chronic compartment
syndrome of the leg in runners. The higher incidence in
motocross is related to the fact that forearm muscles only get
blood flow during relaxation. NASA performed a good study of
forearm muscle blood flow in 1996. While studying normal
volunteers they found "a significant reduction in muscle
oxygenation even at levels as low as 10% maximal contraction."
This explains why we pump up less when we relax, move our
fingers and unclench our hands.
We pump up more on race day because forearm
muscles only get blood flow when they are relaxed.
Nonoperative Solutions to Arm Pump
My research for this article included speaking to numerous
riders and searching both the Internet and the medical
literature. I found recommendations for arm pump ranging from
scientifically accurate to downright bizarre. Since little
true research about arm pump exists, very few of these
remedies have been truly tested. Remember that if a single
person says that after they did X then Y happened, it does not
necessarily mean that Y was a result of X. This concept is how
magic and superstition usually begin. On the other hand, the
mind is a very poorly understood and powerful organ. True
belief in a treatment often has remarkably good results, a
well-documented phenomenon called the placebo effect.
I have broken nonoperative arm pump solutions into three
groups based on the chance of success in reducing arm pump for
a large population. My list does not mean that anything won't
work for you as an individual (see preceding paragraph).
-
High chance of reducing arm pump
- Frequent riding.
- Staying relaxed on the track, loosening the
stranglehold on your grips, moving your fingers, and
alternate between squeezing and relaxing your hands.
- Using more legs and less arms while riding.
-
Medium chance of reducing arm pump
- Avoid heavy weights in arm workouts.
- Suspension set-up.
- Wrist curls with light weights and high repetitions.
- Forearm, wrist stretching.
- Using aspirin as a blood thinner. (The blood thinning
attributes of aspirin work best at low dose. One pill a
day is all you need.)
- Possible chance of reducing arm pump. Treatments that
some riders believed helpful are sometimes diverse and
contradictory:
- Taking nutritional supplements, vitamins, magnesium,
potassium, calcium?
- Changing the bar type, composition, and position (some
say up, some say down) .
- Lever position (some say up, some say down).
- Grip size and stiffness (some said smaller and stiffer
grips helped, while others said a larger softer grip
absorbs vibration and helped.)
- Steering Dampers.
- Gripper seat covers
- Acupuncture
- Magnets
- Voodoo
Operative Solutions to Arm Pump
Surgical release of the forearm fascia (fasciotomy) is
easily performed by an Orthopaedic Surgeon. Fasciotomy is not
a new or difficult procedure and is more commonly performed in
the leg than the forearm. It is often performed in trauma
patients to treat or prevent acute compartment syndrome.
Fascia release consists of first incising (cutting) the skin
and then either incising the fascia or actually removing a
strip of fascia. The four fascial compartments in the forearm
can be released through two incisions. A volar incision to
release the superficial and deep volar compartments, and a
dorsal incision to release the dorsal and mobile wad
compartments.
The use of forearm fasciotomy for arm pump is very poorly
documented in the medical literature. In the few studies that
are written authors contradict one another on several points
including what constitutes abnormal compartment pressures and
which compartments should be released.
Some authors say that a resting compartment pressure over
20 mm Hg is diagnostic for this condition. Others maintain
that an exertional pressure 30mm Hg below the diastolic blood
pressure is important. While still others think resting
pressures greater than 25mm Hg measured five minutes after
exertion is diagnostic.
Similar disagreement exists on which compartments need
releasing. Some authors recommend releasing all four fascia
compartments while others only release those compartments with
elevated pressures. Still others only release the volar
compartments. Some of this confusion stems from the fact that
in the leg fascial compartments have very little
interconnection and therefore complete fascial release
requires release of all compartments. In the forearm good
evidence shows that compartments are often interconnected and
effective release can be accomplished by releasing just the
volar compartments.
No matter which compartments are released, the operation
can be done as an out-patient procedure (no need for overnight
stay). A cast isn't necessary and return to function rapidly
occurs. Training can start about 2-3 weeks after surgery,
and competition 4-6 weeks later.
The Bottom Line
My approach to arm pump is as follows. First try all the
recommendations listed in the nonoperative section above. If
you still have problems you should consider surgical release
of your forearm fascia. Since not all patients improve with
fascial release this step shouldn?t be taken lightly. I
measure compartment pressures after riding to determine which
compartments to release. I am currently seeking volunteers for
a study to address the disagreements listed in the previous
section. With further study and your help we may be able to
eradicate arm pump in our lifetime.
Your Bike |
Similar Functions Between Bike &
Body |
Your Body |
Air
(Gaseous) |
Inflow & exhaust
Carried by |
Blood
(Liquid) |
Carburetor |
Fuel Mixes with Oxygen in |
Lung |
Intake Port |
Fuel/air Mixture
Carried by |
Arteries |
Transfer Port |
Fuel/Oxygen Mix Sent to Final Area of
Combustion by |
Capillaries |
Ignition (Initiates signals that are
Carried by Spark Plug Wire) |
Combustion Initiated or Controlled
by |
Brain (Initiates signals that are
carried by Nerves) |
Outflow Port |
Exhaust Carried by |
Veins |
Exhaust Pipe |
Exhaust Expelled by |
Lungs |
Expansion (Gases push Piston down) |
Burning Fuel Results in Forceful |
Muscle Contraction (Shortening) |
Chain to Rear Tire |
Work Transferred Through |
Tendons to Bone |
What are Tendons?
Since all the muscle fibers in a muscle perform work,
muscles are very bulky and require a constant flow of oxygen.
These factors explain why muscles never cross a joint. If
muscles did cross over joints, then bending the joint would
squeeze the muscle reducing the needed blood flow. To avoid
this problem muscle fibers transform into tendon fibers as
they approach a joint. By the time the muscle crosses the
joint the transformation is complete and it's the tendon that
crosses.
Tendons are thin, strong, white, ropes that connect muscle
to bone. Like muscle, tendons are made of protein rich fibers.
The protein in tendons is a form of collagen that does not
have the ability to contract. Tendons therefore require much
less oxygen than muscles. Tendons, being thin and strong, are
well suited to bending around a joint. Tendons are a great way
to transfer the power of a muscle across a joint to the next
bone. (Ligaments are a similar type of rope-like tissue but
while tendons connect a muscle to a bone, ligaments connect
one bone to another bone.) Muscles are anchored at both ends
to bone, usually originating on one bone, attaching to a
tendon, which then crosses a joint before inserting on another
bone. The combination of a muscle and its tendon is often
called a "musculotendonous unit". Some muscles, like the
biceps muscle in the arm, cross a joint at both ends and thus
have two tendons, one at each end. (See the arm muscle in
figure 2)
Talk Like a Doctor; A Glossary of Buzzwords
Arterial Pressure |
Pressure inside an artery. |
"Arterial pressure is higher than venous
pressure." |
Capillary Pressure |
Pressure inside capillaries. |
"Capillary Pressure is less than
arterial pressure but more than venous pressure." |
Compartment Pressure |
Pressure inside a muscle compartment. |
"If compartment pressure rises higher
than capillary pressure then muscles don't get enough
oxygen." |
Dorsal |
Toward the back. |
"My knuckles are on the dorsal side of
my fingers." |
Extend |
Straighten |
"Extend your fingers and pull the
clutch." |
Fascia |
Tissue around the outside of a muscle. |
"My fascia is tight." |
Flex |
Bend. |
"Flex your fingers around the grip." |
Ischemia |
Painful condition of oxygen deprivation. |
"High compartment pressure can result in
muscle ischemia." |
Necrosis |
Tissue death. |
"Prolonged muscle ischemia can lead to
muscle necrosis." |
Ligament |
Rope like tissue that connects bone to
bone. |
"I tore a ligament in my knee." |
Tendon |
Rope like tissue that connects muscles
to bone. |
"I can feel my tendons in my wrist." |
Venous Pressure |
Pressure inside a vein. |
"Venous pressure is less than arterial pressure" |
Volar |
Toward the front of the body. |
"My palms are on the volar side of my hand." |
Return to Dr. Cohen's Main Page
Return to Top |